
EFFECTIVENESS OF CALCIUM CHANNEL BLOCKADE FOR ORGANOPHOSPHORUS AND CARBAMATE PESTICIDE POISONING-AN OPEN, PRAGMATIC, 3ARM RANDOMISED CONTROLLED TRIAL REPURPOSING TWO WIDELY AVAILABLE LICENSED MEDICINE
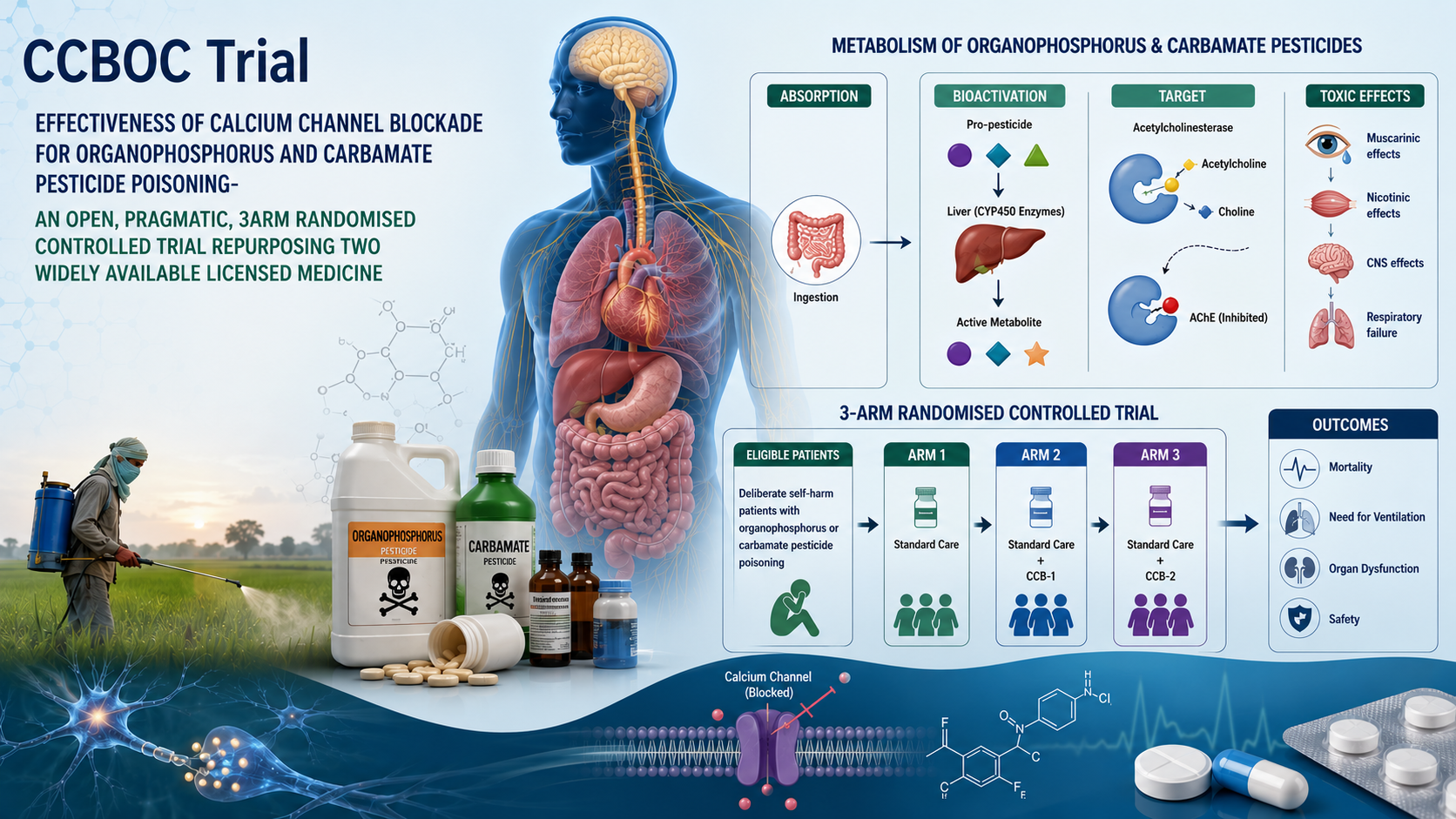
Attempted suicide by drinking pesticides used in farming (called 'pesticide self-poisoning') is the second most important global means of suicide, killing over 150,000 people each year, mostly in poor rural Asian communities. Pesticides called organophosphorus (OP) and carbamate insecticides are responsible for about two-thirds of these deaths. They both inhibit an enzyme called acetylcholinesterase, which usually breaks down the chemical acetylcholine found in the brain and nerves. Because its breakdown is now stopped, acetylcholine accumulates and causes problems with breathing which may kill, even with the best available treatment. Unfortunately, no new medicine has been introduced into medical practice for 50 years, despite thousands of studies and millions of deaths. Current treatment does not always work; new treatments are urgently required. The flow of calcium salt into nerve cells is essential for nerves to work and communicate with other cells in the body. Reducing this flow of calcium with medicines that block channels in the nerve cell - calcium channel blocking medicines [CCB] or magnesium salt - may reduce the pesticides' effects and prevent deaths. Eight studies of magnesium have already been done in poisoned patients; some have suggested benefits from this treatment, but they have been too small and the results mixed.
There is no clear information on whether these medicines work. We propose to set up a multi-centre study (or randomized controlled trial, RCT) of patients with OP or carbamate poisoning admitted to 4 key Bangladeshi hospitals, where this poisoning is a major problem, killing thousands of people each year. We will recruit around 3,243 patients to the study over four years. One- third of the patients selected at random will receive standard treatment, while 1/3 will be treated with additional CCB medicine (nimodipine) and 1/3 will be treated with additional magnesium. The extra treatments will be given for 2 days. We will check how many patients die (currently about 11% die with normal treatment) and how many need to go to the intensive care ward for help with their breathing (called mechanical ventilation where a machine breathes for them) across the three groups. We will look to see whether these additional treatments reduce the number of patients dying or needing to go to intensive care for mechanical ventilation. This study will provide evidence about whether these relatively cheap, widely available treatments help poisoned patients. It might result in the first new treatment for these forms of poisoning for 50 years being introduced in routine hospital practice across the world. The results will be shared with the World Health Organisation and our colleagues in poison centres and hospitals across Asia. Better treatment offers the opportunity to save tens of thousands of lives amongst some of the poorest communities in rural Asia and reduce the heartbreak of suicide amongst children, families, and communities.